 Wednesday · Cardiac & Hemodynamics
Wednesday · Cardiac & Hemodynamics
June 10, 2026
The Number That Lies When It Reads Normal
Why ScvO2, the CO2 Gap, and the Pcv-aCO2/Ca-vO2 Ratio Belong Together at the Bedside in 2026
Read on Substack →Wednesday Edition
Every Wednesday: the physiology that drives every intervention.
Hemodynamic instability is the most common reason patients are critically ill. The vasopressor you choose, the fluid you give (or don’t), and the right ventricle you forgot to assess shape every other decision. Every Wednesday, ICCN publishes a bedside summary on cardiogenic shock, RV failure, vasopressor strategy, and the hemodynamic literature that should change practice.
What This Track Covers
Latest From This Track
Wednesday · Cardiac & Hemodynamics
June 10, 2026
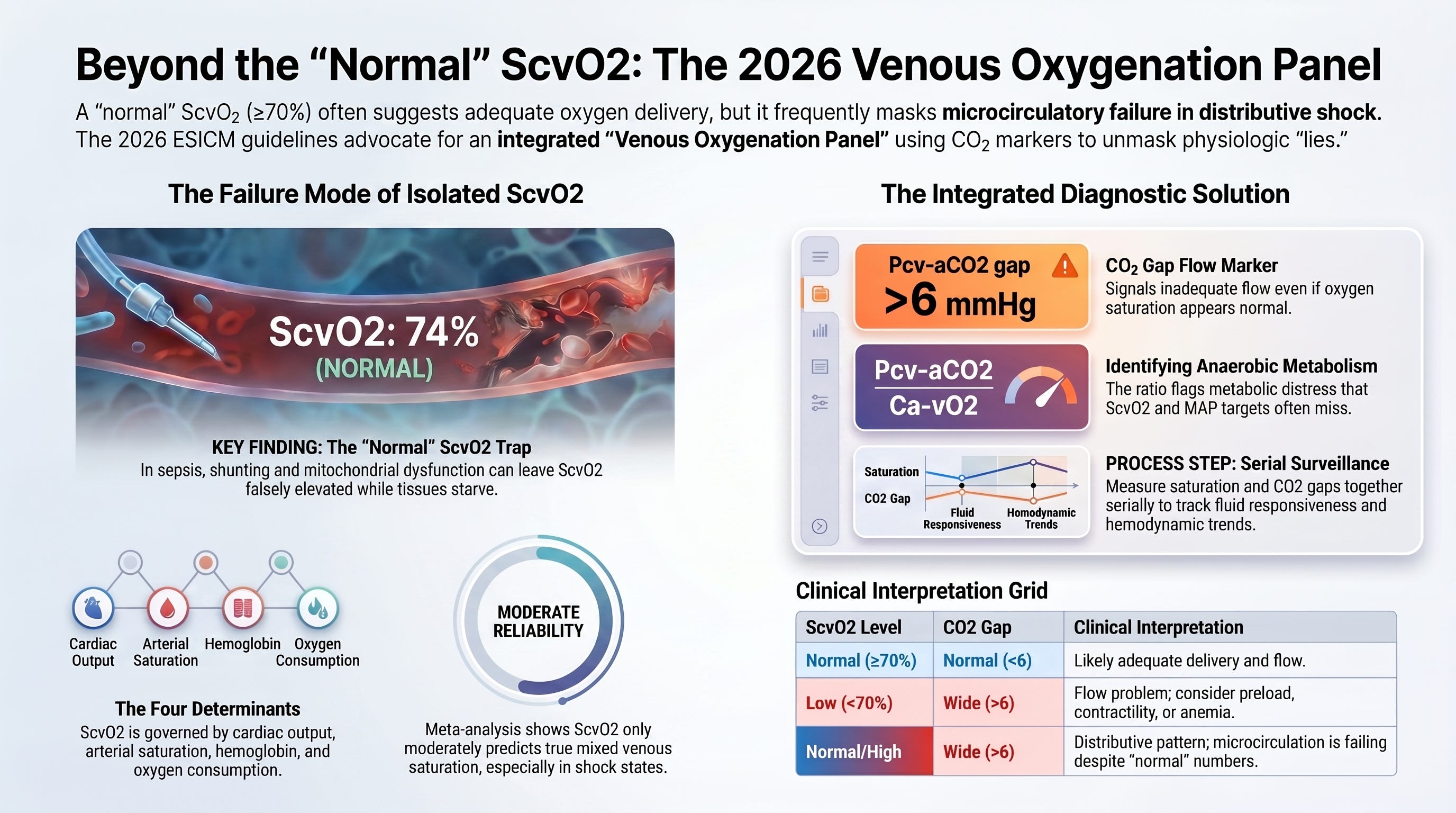
Why ScvO2, the CO2 Gap, and the Pcv-aCO2/Ca-vO2 Ratio Belong Together at the Bedside in 2026
Read on Substack →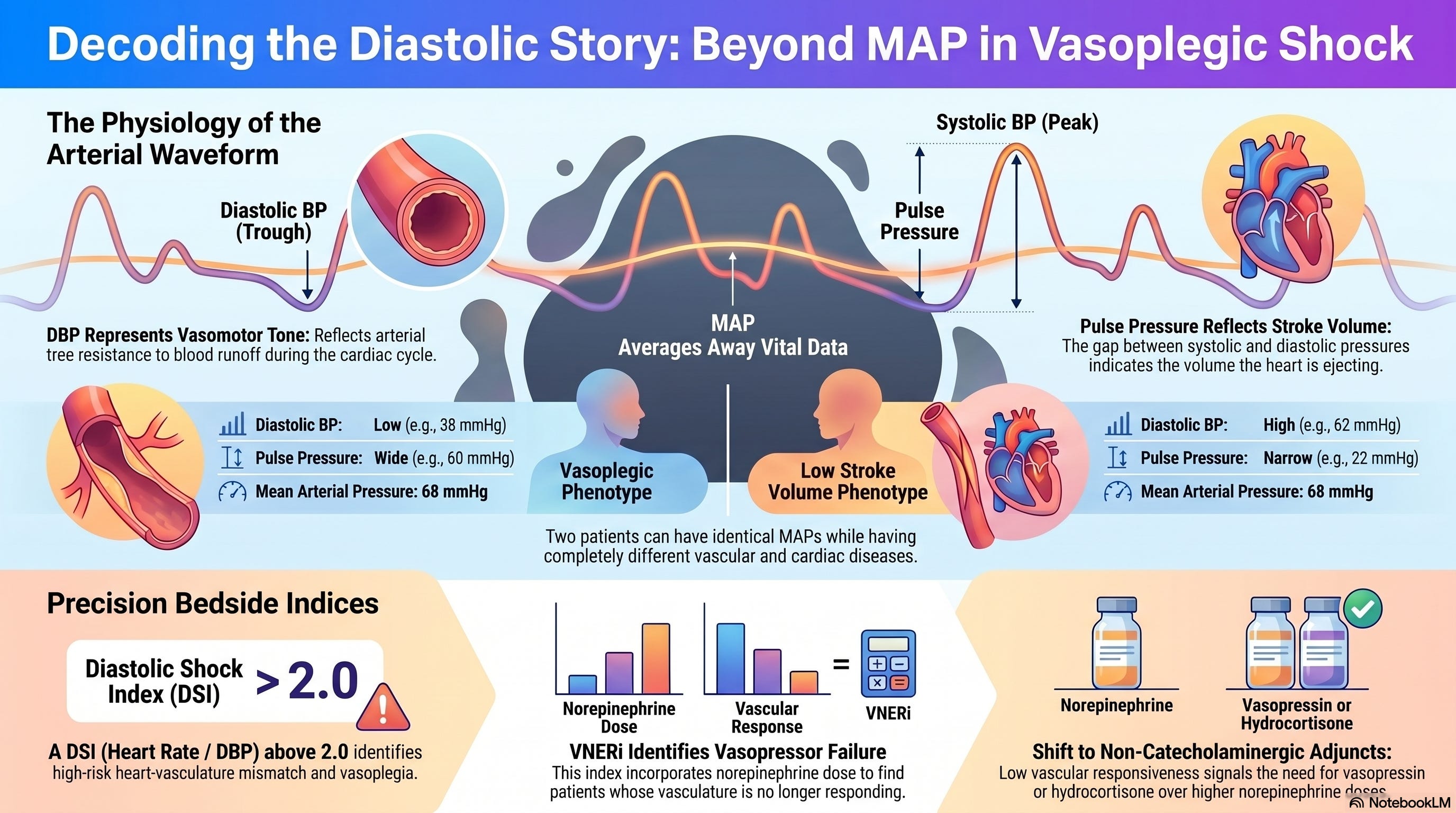 Wednesday · Cardiac & Hemodynamics
Wednesday · Cardiac & Hemodynamics
June 3, 2026
Why DBP, the Diastolic Shock Index, and VNERi Belong on Every ICU Whiteboard in 2026
Read on Substack →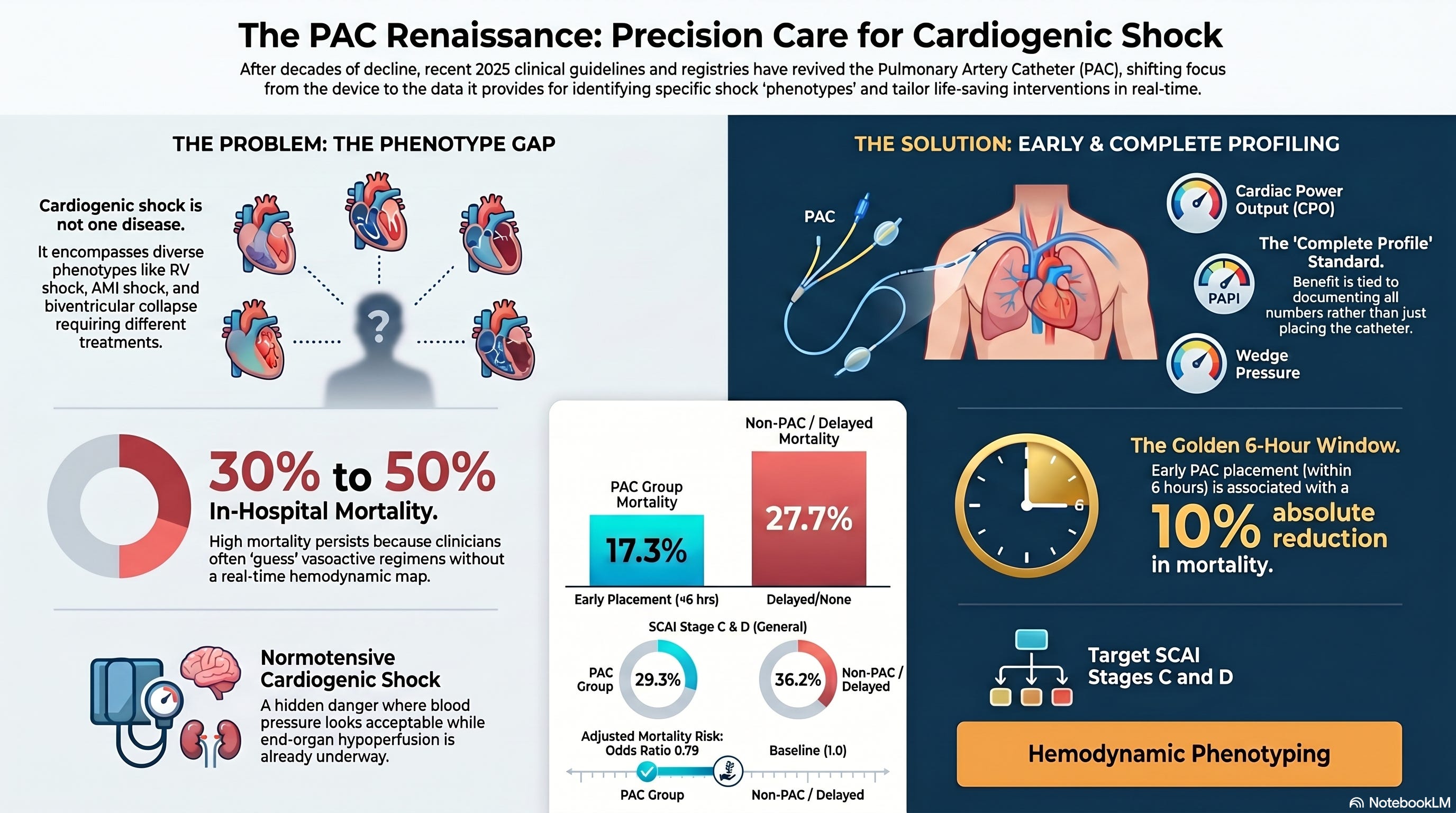 Wednesday · Cardiac & Hemodynamics
Wednesday · Cardiac & Hemodynamics
May 27, 2026
Why the 2025 ESICM Guidelines and Every Major Cardiogenic Shock Registry Are Now Pointing in the Same Direction
Read on Substack →A Note from the Founder
Most ICU decisions are hemodynamic decisions at their core. Understanding why the cardiac output is low — preload, afterload, contractility, rate, or rhythm — is the difference between intervention that helps and intervention that harms.
— Javier Amador-Castaneda, BHS, RRT, FCCM, PNAP
Don’t Miss Wednesdays
Members unlock the full archive across all seven editorial tracks.